
By Lambert Strether of Corrente.
We know that persons with Covid travel on airplanes; the question becomes how to protect ourselves from them — assuming that we our selves are not infected — under conditions of state abandonment such as those prevailing under the Biden Administration (for example, no mask mandates after the airlines and an aggressive minority of passengers successfully discredited their use). The answer given by government experts is that people should perform a “personal risk assessment”. Unfortunately for this paradigm, breathing is a social relation. There is no risk of catching Covid when one is alone. However, since Covid is airborne 40% of Covid infections are asymptomatic, there’s no way to assess risk when one is with others, sharing their air. Thus, the “Personal Risk Assessment” paradigm has the amusing characteristic of being impossible to perform exactly when it is most needed. It follows that one cannot perform a “Personal Risk Assessment” during a flight on an airplane, at least in the general case where one is not sitting next to somebody with a persistent cough. So we must fall back on heuristics. This post will supply many.
My view is that even if Covid is a long-tail phenomenon, the result of my catching it would be ruin, even if the case were not mortal (possibly due to vascular or neurological effects, almost certainly due to financial effects if I end up hospitalized). I think what is true for me is also true for the great majority of the country, so although I may be an outlier in my views, I’m not an outlier on Covid’s potentially ruinous effects.
Hence, my standard for safe air is outside air, as measured by CO2 concentration, the lowest possible (Covid is airborne, and although we cannot measure the concentration of virus, CO2 serves as an adequate proxy, since people breathe it out along with the virus, if they have it.) The USDA sets the baseline:
CO2 levels in outdoor air typically range from 300 to 400 ppm (0.03% to 0.04%) but can be as high as 600-900 ppm in metropolitan areas.
In this post, I’ll see how far the airlines get in meeting my baseline (generously, I’ll take the level of 600-900ppm as acceptable, although 400 is really what I have in mind). First, I’ll look at how the airlines frame their safety concerns (essentially, that ventilation systems make airlines as safe as operating rooms). Next, I’ll look at the realities of safety in the air and on the ground. As we shall see, the airlines’ public relations strategy of focusing on the aircraft cabin is deceptive in a number of ways.
Airline Claims of Safety from Covid
Here is the International Air Transport Association (IATA) on safe air on airplanes:
The quality of supplied air on board an aircraft is much better than most indoor environments. This along with other cabin features including the mandatory usage of masks on board and the requirements around tests and/or vaccination certificates, make the risk of contracting COVID-19 to be very low.
Most modern jet aircraft are equipped with High-Efficiency Particulate Air (HEPA) filters. These filters have similar performance to those used in hospital operating theatres and industrial clean rooms.
These HEPA filters are 99.9+% effective at removing viruses, bacteria and fungi.
(Note the qualification on masks, an impediment to operational efficiency and profit that the airlines have successfully done away with.)
So the claim (oft-repeated) is that airline air is “as clean as an operating theatre.” But it’s not. From “Workplace exposure to carbon dioxide during routine laparoscopy – is it safe?“, here is the baseline for an operating theatre:
During 27 laparoscopies, the measured CO 2 reached a maximum concentration of 1100 ppm, less than one fourth of the LLV. .
Commerical aircraft do not meet this baseline. From “The on-board carbon dioxide concentrations and ventilation performance in passenger cabins of US domestic flights” (2018):
We measured real-time CO2 concentrations, an indicator of ventilation rates, and cabin pressure in the passenger cabins of 179 US domestic flights from boarding through deplaning. and the estimated outside airflow rates were 5.77 ± 2.09 L/s/p across all flights.
Further, the authors make the essential point:
Verification of ventilation performance rather than reliance on design estimates for determining compliance with ventilation standards is recommended.
In essence, IATA is giving us product specifications for their HVAC systems. But we have no data on actual performance. For example, this study, “Is COVID-19 on airplane air filters?“, is only now being done, in 2022. The deck: “Researchers don’t know, but they are looking.” Oh:
With this support, the researchers will specifically look for evidence of pathogens, including SARS-CoV-2, on used filters collected from airplanes. If viruses can be found on filters, then filters from international flights could be used as a new way to track when and where viruses enter the country. Rather than testing travelers individually, it might be possible to monitor entire flights with one test.
(Two years into a pandemic [bangs head on desk].)
Further, there’s reason to believe that the above study is conservative. From CBC, also in 2018:
In the cabins, where the passengers sit, the carbon dioxide levels are much higher. It’s typically , and during boarding, it can get as high as 2,500 ppm, said [Joseph] Allen [of Harvard T.H. Chan School of Public Health]. To give you a sense of what those numbers mean, we can compare them to outdoor carbon dioxide concentrations which are about 400 ppm, while indoor building levels are usually kept under 1,000 ppm.
So there’s no reason to believe that the airlines are meeting the baseline of an “operating theatre” and every reason to believe they are not. In fact, there’s plenty of reason to believe that airlines are doing worse in 2022 than they were in 2018. That’s because today people can measure CO2 themselves with small portable monitors (in what, in optimistic moments, I would characterize as a popular movement). For example:
Not meeting the “operating theatre” baseline (1):
I have an Aranet4 and this has not been my experience. I read the claim that airplanes ventilate, but it’s false. They have the capability – but airflow can be (and is) turned down.
“Airplanes, in particular, have fantastic systems with an estimated 10-20 air changes per hour” pic.twitter.com/ylLP8ApSnW— wildflours (@SeaFlourChild) April 22, 2022
Not meeting the “operating theatre” baseline (2):
Took a flight yesterday. My Aranet4 home CO2 monitor rose above 1,400 ppm during boarding (equates to their highest rating of CO2 levels). Did not drop below 1,400 until we deplaned nearly 3 hours later. Doesn’t seem like airplane circulation is very good…
— LC (@cassidyllc) May 9, 2022
Not meeting the “operating theatre” baseline (3):
Air travel w an Aranet4 CO2 meter. Graphic below is CO2 levels combined w atmospheric pressure. The airplane was close to capacity w HEPA filtration. At cruising altitude, CO2 was ~1500-1700.#airplaneCO2 @AranetIoT @kprather88 @CorsIAQ @DavidElfstrom @Poppendieck @TySopko pic.twitter.com/9pAPWZRnmd
— ChurchAndCovid – Protect Each Other (@ChurchAndCovid) November 8, 2021
Not meeting the “operating theatre” baseline (4):
It was just 1 hour flight and CO2 level never went below 1200 ppm… 😑
It’s still red flag, and – although I trust the air filtration system of the aircraft – I feel sleepy and slightly confused…
–> Why don’t they grant fresher air to people in the cabin?#Aranet4@AranetIoT pic.twitter.com/TR8zKm0CJe— Massimiliano Lo Iacono (@Massimi40945796) July 25, 2022
Not meeting the “operating theatre” baseline (5):
Yes!!! When I showed an @AirCanada airline attendant these ARANET4 readings when everyone took off their masks for beverage service, I could see momentary panic & then complete #Denial.
Told her to tell her shop steward. Unions should be fighting for the health of their workers! pic.twitter.com/6WhltNcSPO
— Elaine Carol (@ElaineCarol3) July 23, 2022
Finally, as it turns out, an aircraft cabin — follow me closely here — is not like an operating theatre at all; that’s an enormous category error. From National Geographic:
About 40 percent of a cabin’s air gets filtered through this HEPA system; the remaining 60 percent is fresh and piped in from outside the plane. “Cabin air is completely changed every three minutes, on average, while the aircraft is cruising,” says Becker. (Lufthansa has a video showing how HEPA filters work.)
Cool tech, but:
HEPA’s 99.97 percent filtration effectiveness sounds reassuring, and airline execs count on that. But the biggest problem with those systems, says Bates, is that the “filter only guarantees the quality of the air that has passed through it. If the air that someone breathes in has not gone through that filter, then those numbers don’t matter.”
In other words, if you’re sharing air with the passenger next to you, and that person is infectious, the HEPA filter will filiter that air only after you’ve already shared it. So, not only are the airlines not meeting the baseline for safe air they themselves have set, the baseline is founded on an incorrect paradigm for how, well, Covid is airborne. Now let’s go into more detail about Covid in the cabin, and Covid at the airport.
Realities in the Air and on the Ground
Let’s back up and assume that aircraft HVAC makes the entire cabin safe. If this claim is true, then two subsidiary claims should also be true: (1) Seating position should not matter, and (2) people should not catch Covid on airplanes. In fact, both are false.
(1) Seat position affects whether you catch Covid or not. This is true in three ways. First, a window seat is safer. From “Covid-19 Risk Among Airline Passengers: Should the Middle Seat Stay Empty?”
We use recent data and research results to approximate the probability that an air traveler in coach will contract Covid-19 on a US domestic flight two hours long, both when all coach seats are full and when all but middle seats are full. The point estimates we reach based on data from late June 2020 are 1 in 4,300 for full flights and 1 in 7,700 when middle seats are kept empty.
Window seat people move about the cabin less, and hence don’t share other people’s air so much:
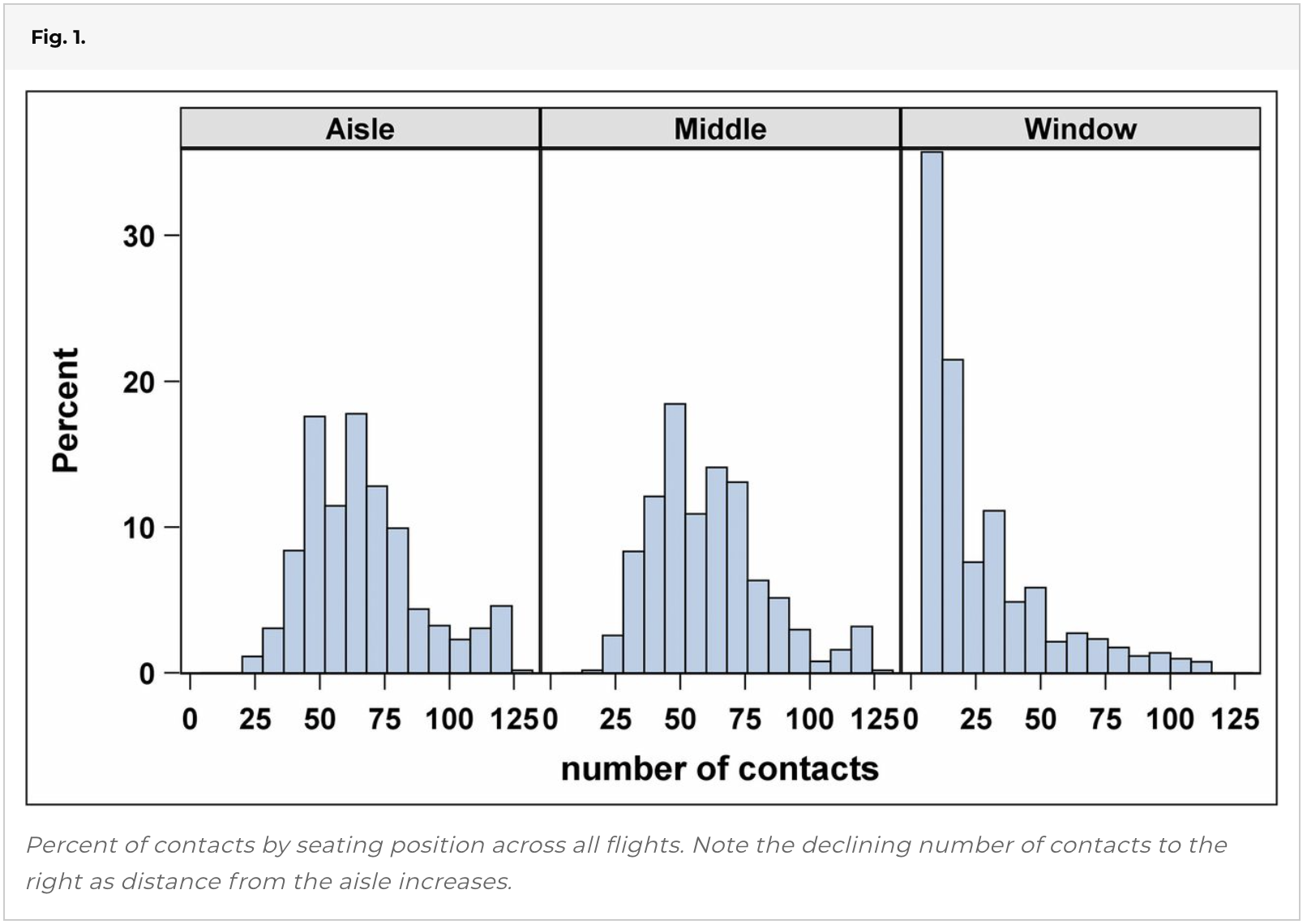
Second, forward is safer than back. From “Inflight transmission of COVID-19 based on experimental aerosol dispersion data”
There is also a clear class difference in the infection probabilities with the FWD (business class) section having much lower infection probabilities than the MID-AFT (economy class) section, which has the highest. The FWD average infection probability is about one-third for the Mild and Medium scenarios and 42% for the severe scenario of the MID-AFT probabilities. These differences are probably due to a number of factors such as lower passenger numbers resulting in greater seating separations and the business class seat geometry possibly offering greater shielding. It is also not clear if the ventilation rate in the business class cabin section is greater than that in the economy class section.
Obviously, air safety in an operating theatre shouldn’t depend on where you stand or sit. The airlines imply that safe air is homogenous through the cabin using diagrams like this:
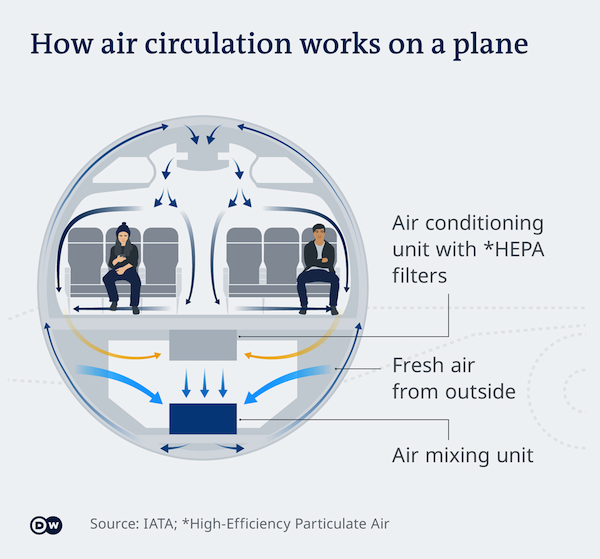
As we can see, this diagram is not helpful, because it doesn’t show that some areas are safer than others.
Finally, as we have already seen, it’s safer when you don’t sit next to infected person (and share their air). From “Transmission of SARS-CoV-2 associated with aircraft travel: a systematic review“:
The evidence from the studies reporting on the on-board transmission suggests that the risk of infection could be higher in individuals seated within two rows of the index cases. Nonetheless, identifying secondary cases seated within a greater distance limits the evidence for restricting the contact-tracing to this area.
Of course, you can’t know your neighbor — say, Bob Wachter — is infected if they’re asymptomatic.
In other words, once again an aircraft cabin is nothing like an operating theatre. Position (window seating; class) matters; the infection status of your neighbor matters; movement matters.
(2) People do in fact catch Covid on airplanes. I can come up with four examples:
• ”Transmission of SARS-CoV 2 During Long-Haul Flight” (London-Vietnam)
• ”A case study of extended in-flight transmission of SARS-CoV-2 en route to Aotearoa New Zealand” (Dubai-New Zealand)
• “A large national outbreak of COVID-19 linked to air travel, Ireland, summer 2020” (Dubai-Dublin)
• ”Assessment of SARS-CoV-2 Transmission on an International Flight and Among a Tourist Group” (Tel Aviv-Frankfurt)
Since the United States has systematically destroyed any ability to do contact tracing, it’s hard to know how many times this has happened. I think that if the medical community saw that four separate operating theatres had an identical infection, Something Might Be Done.
Finally, it would be foolish to take all this precautions in the air, and forget to take precautions on the ground. From the Los Angeles Times late this July:
COVID-19 outbreaks have hit Los Angeles International Airport with at least 400 confirmed cases among Transportation Security Administration staff and workers at American and Southwest airlines, according to county health officials.
At least 233 TSA staffers at LAX have tested positive for the coronavirus since an outbreak was first detected among workers June 9, according to the L.A. County Department of Public Health.
The TSA outbreak would be the largest active outbreak being monitored by the department, which records outbreaks at residential care facilities, workplaces, food and retail stores, homeless service locations, schools, jails, law enforcement settings and courts.
TSA refused to provide current infection numbers, saying it no longer provides such data “because they are consistent with community spread patterns.”
Oh, great. Here’s a quick checklist of items to consider:
1) Transport to and from the airport. If a taxi, open the windows, etc. Don’t take an airport van, there will be more than one person.
2) Movement within the airport.
Queues. Obviously, mask up, social distance if possible, try to time matters to avoid crowds, etc.
Ticket counter
Passport control
Security
Waiting area
Jetway
3Cs spaced (Closed Spaces, Crowded Spaces, Close Contact Settings)
Bathrooms. Use one furthest from the gate, not nearest, i.e. uncrowded.
Food courts and bars. Don’t.
Shops. Don’t
Boarding/Deplaning. You don’t have to board when they call you. Board to avoid the crowd. You don’t have to stand up and get your luggage when the plane stops at the gate. Wait ’til almost everyone has left.
Other tips and tricks will doubtless occur to readers. Please share.
Conclusion
If I were flying, I’d take First or Business Class if I could, I’d take a window seat, I’d go the full Darth Vader on my mask (a step up from my beloved 3M™ Aura™ 9210+) , I’d make sure I had my throat and nasal sprays, and I’d try to avoid being served meals and beverages (I could probably sit and chow down nutrients and liquids in isolation with good timing). I would minimize my movements through the cabin. I would also bring a CO2 meter. And if I had to smile, I’ll crinkle my eyes.
NOTES
[1] We have done such testing for other respiratory viruses, but not for SARS-CoV-2. Is this really too much to ask?


{kind=link}