
By Lambert Strether of Corrente
“Never doubt that a small group of thoughtful, committed citizens can change the world; indeed, it’s the only thing that ever has.” –Margaret Mead
Despite the sound of distant trumpets — “we few, we happy few” — in the epigraph from Margaret Mead, masking remains one of the layers of protection (the “Swiss Cheese Model“) used by many Americans to protect themselves from the neurological and vascular effects of SARS-CoV2, which seem to defy treatment. From the New York Times:
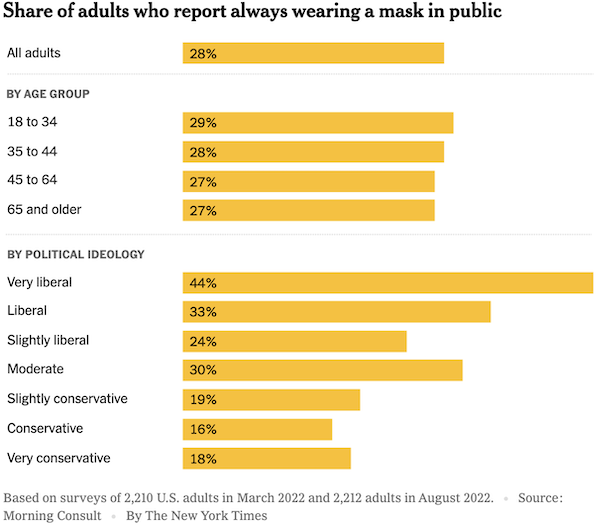
28% of all adults is not a negligible number. (Sadly but typically, the Times didn’t categorize its subjects by income or occupation.) Dominant it’s not, but there are more committed mask wearers, especially in this environment, than there were, say, Volkswagen Beetle owners, back in the day when we’d wave at each other on the road. There are far more mask wearers today, and far more ability to fraternize. Organize, even (as the Corsi-Rosenthal box builders seem to have done, interestingly).
An Op-Ed in the Los Angeles Times, written after our absurdist President’s Ionesco-like remark that “the pandemic is over,” presents one way forward:
Ordinary Americans who cannot afford to be ill — and that is truly tens of millions of us — now have to appeal directly to America’s working medical professionals:
Please make your medical offices safe for us to enter by using N95 masks and top-rated HEPA air filtration. Too many of us are at risk to become severely ill, develop chronic illness or die if we catch COVID, even if we are newly boosted. Just as importantly, many of us are the sole caretaker for someone else, people who depend on us for their everyday needs. We are desperate to avoid getting sick for their protection as well as our own. And the reality is that healthcare providers, run ragged after the last three years, can’t afford to get sick either.
Crucially, we cannot let infectious air be so prevalent that people delay going to a hospital in an emergency because they fear catching COVID there…,
I am speaking directly to our doctors, dentists, nurses, specialists of every kind, all our providers of routine and critical care: In the absence of any backup from government officials, we need your help now. We need to be able to come into your offices for the checkups you always nagged us to keep up with — and we want to get. As your patients, we need a professional commitment from you to practice good infection control.
If you cannot see your way to having everyone inside your office, staff and patients alike, to wear an N95 or equivalent mask all day, please at least create some hours every week when that is the rule for everyone — a required masking portion of the day. Offer this as an option when patients call to make an appointment.
Medical examining rooms and waiting rooms are often windowless. To support masking efforts, get HEPA filters, which are affordable for offices and effective at capturing COVID particles from the air.
And if you understand how much we value our health, if you are among the medical professionals who have been grieving over the nation’s pandemic failures, if you remain committed to preventing infections, please work with colleagues inside your prestigious professional associations to promote clear and effective infection control standards. Your patients can’t do this. The CDC made clear it no longer will. But we hope you can.
I agree with the sentiments and the point of attack, and I think that medical professionals are not as heartless as they are often depicted in anecdotes on my Twitter feed (many of which I repurpose here). I do think that marketing collateral would be needed, along with an FLCCC-like organization. We’ll see. (Of course, what would be really helpful is a public relations campaign — propaganda does work, as we know from current events — on the national scale from a government not dominated by eugenicist views, but we are not at that point, now.)
This post will be a little bit of a smorgasboard. Covid is, in my view, by no means over, even it has plateaued. Nevertheless, the press of awful events to be chronicled has diminished, leaving time to consider topics that we blew past, or which only recently emerged. This post will consider three: mask fit, mask manufacturing, and masks on the movie set (where compliance is near 100%).
But first, let me quote a new study from the American Journal of Preventive Medicine, “Modeling COVID-19 Mortality Across 44 Countries: Face Covering May Reduce Deaths,” and never mind that I hate that locution “face covering”[1]:
This study examines a hypothesized association of face-covering mandates with COVID-19 mortality decline across 44 countries in 2 continents.
In a retrospective cohort study, changes in COVID-19‒related daily mortality rate per million population from February 15 to May 31, 2020 were compared between 27 countries with and 17 countries without face mask mandates in nearly 1 billion (911,446,220 total) people. Longitudinal mixed effect modeling was applied and adjusted for over 10 relevant demographic, social, clinical, and time-dependent confounders.
Average COVID-19 mortality per million was 288.54 in countries without face mask policies and 48.40 in countries with face mask policies….
The results of this study show a significant association between face mask mandates and reductions in COVID-19 mortality. This evidence supports the positive impact of face mask policies on saving peoples’ lives.
Marketing collateral this is not. But it could certainly be converted! (Perhaps the Brains Trust will weigh in on the methodology, which is a bit above my paygrade.)
Wiith that, let us turn our our maskstravaganza.
Mask Fit
I really should have thought of this [slaps forehead]:
I’ve been trying to explain this for two years now. N95s were designed primarily for male caucasian faces. KN95 and KF94 standards came about not because we wanted a knockoff mask standard, but because Asian faces could not pass fit tests with N95 masks. https://t.co/uUkXVXkPXv
— Naomi Wu 机械妖姬 (@RealSexyCyborg) September 27, 2022
And some advice:
The takeaway is mask fit over everything, check with @masknerd for the best ones to try with tested filtration, stick with whichever of those has the best fit.
— Naomi Wu 机械妖姬 (@RealSexyCyborg) September 27, 2022
Of course, if there were some sort of size standard, like there is for shoes, say, we would have to rely less on anecdotal exchanges on Twitter threads. Perhaps the brain geniuses at CDC could create one[2].
Indeed, one would think that the Diversity, Equity, and Inclusion DEI industrial complex could be focusing on centering masks for Asian and Black (and not merely White) faces, instead of spending their time rooting out micro-aggresions and so forth (unless, of course, you consider breathing air polluted by an infectious pathogen a micro-aggression). The DIE DEI folks have a lot of clout in industry and academia, so what say? Save some lives?
The Bill of Health Blog makes the point better than I can, centering the disabled: “The Mask-Optional DEI Initiative“:
Recently, I remotely attended a mask-optional, in-person meeting where campus leaders proudly proclaimed that DEI (diversity, equity, and inclusion) is my college’s “top priority.”[3]…
I should be clear here that this was not specifically a meeting focused on DEI work, but a required department meeting where we were, once again, reminded of this strategic priority by leaders from outside the department. I should add, too, that “access” to the meeting via Zoom only existed because my department chair continues to provide it against a clear university expectation that everyone but those with “approved” accommodations work in-person.
My employer, like many universities, has followed a pandemic trajectory from remote work, to in-person work with masking and vaccine requirements, to in-person work that closely mirrors 2019, except for a small number of people at the institution “electing” to still mask.
Campus buildings — where in-person work is once again the norm — are now adorned with signs that declare with what feels like an overly proud tone that “masks are not required in this building.” And it’s both the moving on from still-necessary, effective, proven mitigations, and the tacit celebrations that such moving on has occurred (as perhaps demonstrated by the tone I read into that sign), that make me question what the managerial performance of an “investment” in DEI is meant to achieve.
I will be direct: .
Moreover, the rejection of masking as a necessary mitigation will continue to prolong the pandemic and increase its harm for everyone, and especially for disabled students, staff, and faculty at institutions of higher education (a population that is likely increasing, for we do not yet know the pandemic’s full harm nor have we curtailed uncontrolled viral spread).
While the ongoing purposeful exclusion and/or harm of disabled students, staff, and faculty is certainly not the first illustration of hypocrisy being hardwired into many DEI performances, it is clear evidence that many institutionally-sponsored DEI initiatives project a better future largely divorced from the current material reality and organizational culture that necessitates “improvement.”
(I would ask also about ventilation.) But where’s the lawsuit? Meanwhile, “an ongoing commitment to purposeful exclusion” seems a little gentle. Why not use the original German, Lebensunwertes Leben? Because society-wide, that’s what the policy amounts to.
Mask Manufacturing
From the New York Times in March 2022, “Why American Mask Makers Are Going Out of Business” (example; example):
It is hard to know precisely how many of these [small American mask manufacturing] companies were born during the pandemic; 36 of them are members of the American Mask Manufacturer’s Association, which they formed to lobby Washington. Virtually all experienced [a] same boom and bust phenomenon,,, At first, customers who could no longer obtain masks through their normal supply channels were beating down their doors. The same was true during the Delta and Omicron waves, when masks were also scarce.
But as soon as the waves crested, and Chinese companies, determined to regain their market share, began exporting masks below cost, the customers disappeared.
The government’s answer to this pattern is its own buying power. During his State of the Union address on Tuesday night, President Biden promised that the government would begin to rigorously enforce provisions in the law that call for the federal agencies to buy American-made goods whenever possible.
The plight of these small mask companies, however, suggests that reviving American manufacturing — even when the underlying rationale is national security — won’t be easy.
“Resilience is the byword of the day,” said Marc Schessel, a hospital supply chain expert who is working to develop alternative supply chains for personal protective equipment. And resilience — that is, creating extra manufacturing capacity that can get the country through an emergency — is what the small mask makers say is their value to the country.
Wait. Schessel is a supply chain experts. That means he wants to optimize the chain so that there’s no slack or inventory; “tight coupling” as Yves calls it. But we don’t have to accept that model. Why can’t we put masks into inventory? (Good masks that, America being diverse, fit all faces.) More:
The mask manufacturers I interviewed for this article said the Biden administration had expressed interest in buying their masks, but it has yet to happen. Even if it did, it would be unlikely to put much of a dent into Chinese dominance. As Mr. [Mask Manufacturer] Bowen put it in a recent email to the White House, “Hospitals drive the mask market.” Since their incentives are to reduce costs, he wrote, “Any plan that allows imported masks to cost less than U.S. made masks will result in a foreign government controlled U.S. mask supply — as currently exists.”
To put it another way, the modern imperative of maximizing shareholder value will always put efficiency and cost over resilience.
That’s an interesting perspective on the priorities of our ginormous monopolized system of hospitals[4], isn’t it? There’s no consideration for the health of patients and health care workers at all. How do these hospital buyers sleep at night? The article concludes:
Despite the president’s vow to have the government buy American, the most likely scenario remains what it has been for months: the small mask manufacturers will go out of business, hospitals will continue to import Chinese masks — and the country will again be caught short when the next pandemic arrives.
Plus ça change….Because we’re not a serious country.[5]
Masks on the Movie Set
The film industry is different:
Public: eating/partying indoors is fine. Just get your booster if you want. You do you.
Film/TV industry: test, vax, measure CO2, isolate, quarantine, ventilate, mask when not on camera, clean the air. No exceptions.
— Debbie Winslow (@Debbie_Winslow_) September 23, 2022
Here’s what one contractor does:
We aim for CO2 less than 1000ppm, and if we can’t get there, we introduce HEPA/air scrubbers/air movers into the stages/sets. Here are examples of what I did for some productions. pic.twitter.com/NqoBsNZyiS
— Erin Bromage Ph.D. (@ErinBromage) September 22, 2022
1000 is a little high, to my mind, because my rule of thumb is outdoor air. Another:
— Lazarus Long (@LazarusLong13) September 21, 2022
But why? Why, you ask? Why does a crazy industry like Hollywood have such good protections for workers, and my workplace — or college, or hospital, does not? The answer:
Think masking is for idiots?
This thread is for you.
In what industry are people considered to be THE assets?
Doctors. Lol. Wrong.
Bankers? Ha!
Teachers? Bwahaha!Actors.
— Lazarus Long (@LazarusLong13) September 21, 2022
“The talent” is not expendable. But you are (unless you believe that labor is the source of all value, which puts a different spin on who’s expendable, but that is a topic for another time).
Conclusion
I’d like to conclude by kicking CDC’s twitching corpse a little, but I’m not yet ready to look at 3M’s respirators, designed in 2008 for a pandemic situation just like our own, and why CDC never recommended their use.
Instead, I’d like to close with a look at trust (or, I suppose, if we wish to be modern, “pro-sociality”). From STAT, “The CDC’s latest blunder is really about trust, not masks“:
The bigger concern here is not with what the CDC actually said, but with the fact that there is a deep lack of trust in our society. People don’t feel like they can rely on one another to follow guidelines that aren’t enforced with mandates or penalties. And while there’s good reason for why that trust has evaporated, the CDC’s choice to release or withhold information to us all should not depend on whether some people might abuse that information. The public deserves to be told the truth about where the science stands; the public also deserves competent governors and public health department chiefs who can communicate nuance and decide what policies make sense to implement at a community level.
There’s no question that trust must be rebuilt between members of the public, and between the public and health agencies and leaders. But for this to happen, we must all acknowledge that the lack of trust is what’s bothering us.
For now, at least until we can get that 28% figure higher — masks work for the flu, colds, and childhood respiratory diseases, too — or at least stomp the mocking and policing and smile-extortion, we might give consideration to treating masks as a trust marker. A mark of solidarity, if you will.
NOTES
[1] I hate pseudo-scientific locution “face covering” because it’s false: The eyes (“the windows to the soul”) are not covered by masks, and last I checked the eyes were part of the face, at least for humans. Indeed, most mask designers, when constructing their use cases, seek to avoid such scenarios as users walking into walls, into traffic, falling downstairs, etc.
[2] I doubt that a standard as simple as shoe sizes could be constructed for “mask fit”; see the fitting process here, for example. But we could surely do better, such that half the globe isn’t left out by the parameters we think are universal, because they apply to us!
[3] What, not even fundraising?
[4] I have not looked at the Center for Disease’s standards guidance for its hospital infection control material. If CDC guidanceon masks is as horrid as its guidance on airborne transmission, it will be optimized for cheap-jack, non-functional Chinese goods bought in bulk for pennies.
[5] There is also, apparently, a large contract with big manufacturers like 3M. That way, giant hospital monopolies can purchage from giant manufacturing monopolies. All fine, I suppose, except if there’s one thing mask manufacturing needs, it’s real innovation — not just for fit, but as I keep screaming, for fashion* — and giant monopolies just don’t do that. NOTE * For example: Why on earth don’t we sell masks to school children with stickers? Kids love stickers, or did in my day. And so on, and so on.


{kind=link}